You’ll find quick answers here to our most commonly asked questions, with links to where you can find out more.
Group B Strep Support can provide general information on group B Strep, but cannot give you advice, nor counselling or a diagnosis. If you need medical advice, please contact your health care professional.
Group B Streptococcus (Group B Strep, Strep B, Beta Strep, or GBS) is a type of bacteria which lives in the intestines, rectum and vagina of around 2-4 in every 10 women in the UK (20-40%). This is often referred to as ‘carrying’ or being ‘colonised with’ GBS.
Group B Strep is not a sexually transmitted disease. Most women carrying GBS will have no symptoms. Carrying GBS is not harmful to the carrier, but it can affect your baby around the time of birth.
Carrying group B Strep has no symptoms, so testing is the only way to find out if you are carrying the bacteria. A group B Strep test is simple, safe and effective.
If a women is known to carry group B Strep in her current pregnancy then she will be offered antibiotics from onset of labour which will minimise the risk of her newborn baby developing a group B Strep infection. Group B Strep is the most common cause of infection in newborn babies causing meningitis, sepsis and pneumonia.
At present, not every pregnant woman in the UK is offered testing for GBS on the NHS. If you are offered a test on the NHS it’s very important to find out which test they’re using as not all tests are equally reliable. If you are unable to be tested on the NHS using the GBS-specific Enriched Culture Medium (ECM) test, you can opt to pay for this privately (click here for information about private ECM tests).
If you would like to be tested for GBS, talk with your midwife so you can discuss the options available on the NHS first. If you decide to order the test privately, most women would aim to test within the last 5 weeks before they are due to give birth (between 35-37 weeks’ of pregnancy).
You can test earlier in pregnancy, but the test result is not as reliable at predicting what your carriage status will be (positive or negative) when you give birth. The test can also be done later, but the chance increases that the baby will arrive before the test result does. If you have a history of going into labour early or are expecting twins (or more), you may want to take this into account when doing your group B Strep test.
You can find the latest availability of the ECM test from private suppliers listed at www.gbss.org.uk/test.
The charity does not sell ECM tests, but signposts to reputable organisations that do.
One of the easiest ways to do a group B Strep test is to order a DIY testing kit from a supplier offering ECM tests. They cost from around £38 and payment will need to be made directly to the company and not the charity. The test result is sent to you within 3 working days of the company receiving your swabs (usually initially by text).
You will receive your result by text as soon as it becomes available. A paper copy should then follow in the post, which can be added to your medical notes. (Until the paper copy arrives, it might be helpful to keep a screenshot of the results text.)
Remember, if you are chasing up your test results, you will need to contact your test kit provider to find out where your test or test result is.
All test providers listed on our website supply the internationally-recognised ‘gold standard’ ECM test for GBS as recommended by Public Health England.
You can find contact details of the testing companies here www.gbss.org.uk/test
The ECM test is a home test pack that is safe and simple to do yourself. And each of the test packs includes clear instructions. It involves a low vaginal swab and a rectal swab.
Reliability of the test, depends which test you’re using.
The tests widely available in the NHS (the standard direct plating tests) are not very reliable when they give a negative result – they give a negative result up to 50% of the time when they should be positive. On the other hand, a positive conventional test result is very reliable (they rarely find something that’s not there). For more information on different types of group B Strep tests please see our page: https://gbss.org.uk/info-support/group-b-strep-testing/different-types-of-tests/
The GBS-specific ECM (enriched culture medium) tests are highly reliable and are good predictors of your GBS carriage status for 5 weeks after the swabs have been taken. A number of NHS trusts offer the ECM test to some or all pregnant women, together with private sources, including home-testing packs, which you can find details for here: https://gbss.org.uk/info-support/group-b-strep-testing/ecm-test-where-how/.
If you are taking antibiotics, or have recently, this may affect the test result so discuss this with your midwife or doctor. If you can, leave it for a couple of weeks after completing the antibiotics before testing.
Your normal vaginal and rectal flora should begin to normalise a week after finishing the course of antibiotics. Ideally, there should be a gap of at least 7-10 days between finishing a course of antibiotics and taking the ECM test for GBS carriage.
If you have been using an anti-fungal pessary and want to test for group B Strep carriage, it would be prudent to finish the course of treatment and then wait two days (or longer) before taking the vaginal and rectal swabs for the ECM test. The reason for this is that some anti-fungal agents, for example clotrimazole, have some effect against gram-positive organisms such as group B Strep.
No. Research has shown that, whatever the result of a sensitive test for GBS carriage, your status is hugely likely to be the same for the next 5 weeks. After that, the predictiveness wanes a bit – though it doesn’t plummet like a stone.
The research also found that, for the group B Strep specific ECM test done in the last 5 weeks of pregnancy, a negative result was 96% predictive of not carrying GBS at delivery (4% of women acquired carriage between the test and giving birth) and a positive result was 87% predictive of carrying GBS at delivery (13% of women lost carriage between performing the test and giving birth). This is why testing is recommended in the last 5 weeks before the anticipated delivery date. This is usually at 35-37 weeks of pregnancy – so the results remain predictive for when you are most likely to give birth and the test result should be available before your baby arrives.
Some of the confusion of UK health professionals may be because the standard NHS swabbing method (high vaginal swabs, or HVS) and culture method (direct plating) were not designed specifically for detecting GBS and are not great at finding it. Research has found these methods will miss up to 50% of the women carrying GBS at delivery. Clearly a positive test result obtained by this method is highly reliable, but if you get a negative result, you can’t be sure it’s because the GBS isn’t there or whether the test simply didn’t detect it.
Not all NHS trusts offer the ECM test yet (although it’s recommended for use for detecting GBS by the Royal College of Obstetricians), but they are available privately from around £38. See www.gbss.org.uk/test for the latest availability.
The reliability of a negative result from a test for group B Strep carriage depends on the timing of when the samples were taken, where the samples were taken from, and what method was used to process those samples.
- A negative group B Strep result from an ECM test is highly reliable. Research has found that, when the ECM (Enriched Culture medium) test was properly performed within 5 weeks of the mother giving birth, a negative result was 96% predictive that she would not be carrying group B Strep when she gave birth (so only 4% of women acquired GBS carriage between the test and giving birth).
- A negative group B Strep result from a standard NHS swab test, however, is not reliable – this test gives a high proportion of false-negative results. This test only finds group B Strep about half the times it is present, so around half (50%) of those carrying group B Strep will be incorrectly told they are not.
If you have tested negative using the ECM test, the result is highly reliable for the next 5 weeks. Please do discuss the results with your midwife and healthcare professionals to discuss your options and whether you would prefer to choose to have IV antibiotics in labour.
A positive test result is highly reliable. Any positive test result (NHS or private) is a very strong indicator that GBS was present when the samples were taken. It is very unlikely that a test will give a falsely positive result (i.e. finding group B Strep when it’s not present). All UK national guidelines recommend that Mum should be offered intravenous antibiotics in labour if GBS has been detected during the current pregnancy. Please do let your midwife know you have tested positive for group B Strep and discuss your planned place of birth with them.
Our page: https://gbss.org.uk/info-support/about-group-b-strep/what-is-group-b-strep/ should answer most of your questions about GBS during pregnancy as well as our page on decisions to make after testing positive: https://gbss.org.uk/info-support/group-b-strep-testing/what-does-my-test-result-mean/
If you’d like a ‘GBS Alert’ sticker for your hand-held pregnancy notes, ping us your postal address and we’ll get a couple in the post to you – they’re a good visual reminder about the intravenous antibiotics recommended once you go into labour, or your waters break to minimise the risk of GBS infection to your baby.
It is only after waters break or labour starts that the IV antibiotics given to women known to be carrying GBS have been shown to be effective at reducing the early-onset group B Strep infections – you couldn’t (and wouldn’t want to) attach a woman to an IV drip for weeks on end just in case her labour was about to start.
Oral antibiotics are usually only prescribed when GBS is found in your urine. Taking a course of oral antibiotics as a method of prevention is not recommended as it won’t get rid of colonisation in the vagina and intestines.
Evidence shows taking antibiotics before labour does not reliably eradicate GBS carriage – and there’s no evidence that it reduces the incidence of GBS infection in newborn babies either. The time when the antibiotics are effective against GBS infection in newborn babies is when they’re given in labour.
Some women may experience temporary side effects, such as feeling sick or having diarrhoea. Women can be allergic to certain antibiotics and, in rare cases, the reaction may be severe or even life-threatening (anaphylaxis). However, this is very rare – in the USA between 1997 and 2001, an estimated 1.8 million women were given penicillin in labour and no deaths from anaphylaxis were reported.
Please do tell your doctor or midwife if you believe you are allergic to penicillin or any other medications.
There are always risks associated with taking any medication, including antibiotics. Research has shown that intravenous antibiotics (ideally penicillin), given in labour to women whose babies are at higher risk of developing GBS infection, is highly effective at reducing the risk of GBS infection in newborn babies, without any known long-term side-effects on the baby, and no apparent tendency to increase antibiotic resistance. Indeed, GBS has remained sensitive to penicillin for over 60 years.
If you have any concerns about the effects of the IV antibiotics, please speak to your doctor or midwife. Your doctor or midwife should discuss with you both the benefits and the risks of taking IV antibiotics in labour to prevent early-onset GBS infection in your baby.
If you’re being offered intravenous antibiotics in labour against early-onset GBS infection (developing in babies aged 0-6 days), these should be started as soon as possible once labour starts or waters break at term. Although it’s not likely to be an issue, do press your health professionals to start the IV antibiotics as soon as you think you are in labour, if you need to.
Research has shown that having the first dose 4 or more hours before the baby is born (and having them at regular intervals until the birth) is highly effective at preventing early-onset GBS infection.
Although not as protective as 4+ hours before the birth, having the first dose of the IV antibiotics 2+ hours before your baby is born should provide significant reassurance. The IV antibiotics actually start crossing to the baby within minutes of being given, building up over time to reach therapeutic levels in the baby, so almost anything is better than nothing.
If you are very anxious about giving birth before you receive adequate IV antibiotics, please speak with your Consultant Obstetrician, who will be able to give you medical advice based on your specific circumstances. Neither of the options below are routinely recommended by our medical advisory panel, though if you are really concerned, you might like to discuss them with your Consultant Obstetrician.
If you receive the first dose of IV antibiotics less than 4+ hours before your baby is born, the guideline against early-onset GBS infection recommends your baby should be monitored for their first 12 hours of life.
If group B Strep was detected in your previous pregnancy and your baby did not develop a group B Strep infection, there is a 1 in 2 (50%) chance that you will be carrying group B Strep again this pregnancy. To help you choose whether you would like to have IV antibiotics in labour, you can have a specific swab test (known as the Enriched Culture Medium or ECM test) to see whether you are carrying GBS when you are 35-37 weeks pregnant.
Clinical guidelines recommend that you should be offered this ECM test by the NHS, but we know that some NHS hospitals do not yet offer ECM tests. If your hospital is unable to offer ECM testing, you may choose to purchase an ECM test privately.
If the result shows that:
- you are carrying group B Strep, then the risk of your baby developing early-onset group B Strep infection is increased to around 1 in 400 and you will be offered IV antibiotics in labour.
- you are not carrying group B Strep, then the risk of your baby developing early-onset group B Strep infection is much lower (1 in 5000) and you may choose not to have IV antibiotics in labour.
A positive urine culture test result is highly reliable at finding GBS in the urine. When GBS is found, depending upon the level of bacteria found and whether the Mum has any symptoms, Mum may be treated with oral antibiotics at the time of diagnosis. Intravenous antibiotics would also be offered when you go into labour.
GBS detected in the urine does not always mean an infection is present, particularly when the level detected is low – sometimes it is just that the urine has picked up some of the bacteria from vaginal GBS carriage on its way out of the body. If the Mum does not have a GBS urinary tract infection, then treatment is not usually recommended at the time it’s found.
Treatment for GBS detected in the urine depends both on the level of GBS found and whether or not you have any symptoms. It’s best to speak with your health team about this. If treatment is recommended for GBS bacteria in the urine during pregnancy, oral antibiotics are given, usually for 5 days.
Read more about GBS being detected in the urine here.
If you are not currently pregnant but want to find out more about GBS, please see our page for more information.
Our medical advisers do not recommend induction for anyone as a way of combating GBS infection in babies. Carrying GBS, or your baby being at raised risk of GBS infection is not a reason to be induced.
However, you should be offered immediate induction plus the intravenous antibiotics in labour if you are known to be carrying GBS and your waters break before labour starts, because of the increased risk of early-onset GBS infection developing in babies after prolonged rupture of membranes.
If you live a long way from the hospital or have a history of very fast labours, induction may be one way to try and ensure you get sufficient intravenous antibiotics in labour. However, induction is not without risk itself, especially before the due date. You should discuss the potential risks and benefits of induction with your obstetrician because they will vary dependent upon your personal circumstances.
If you need to be induced, the recommended intravenous antibiotics should be started as soon as possible once labour has started or waters have broken (naturally or artificially) and should be repeated 4-hourly (for penicillin) until your baby is born, and ideally for at least 4 hours before delivery.
Caesarean sections are not recommended as a method of preventing GBS infection in a baby. They reduce but do not eliminate the risk of GBS infection to the baby, since GBS can cross intact amniotic membranes to cause infection in the baby. There are also risks associated with Caesarean sections; plus the recommended intravenous antibiotics during labour are highly effective and low risk.
If however you are having a Caesarean section, our medical panel’s recommendations with regard to GBS are as follows:
Elective Caesareans There is no evidence to show intravenous antibiotics are indicated against GBS when a woman is known to carry GBS or who previously had has a baby infected with GBS is having an elective Caesarean unless she is in labour or her membranes have ruptured. If a baby is at higher risk of developing GBS infection and the mother is having an elective Caesarean AND is in labour OR her waters have broken, she should be offered the recommended intravenous antibiotics as soon as possible after the start of labour.
The baby would only need intravenous antibiotics against GBS infection if born prematurely or if there are signs of possible infection in either the mother or the baby.
Emergency Caesareans If a woman carries GBS or has previously had a baby infected with GBS and needs an emergency Caesarean, she should be treated as for an elective Caesarean – no intravenous antibiotics are indicated against GBS unless she is in labour. If she is in labour, she should be treated as for normal labour up until the time when an emergency Caesarean section becomes necessary, when she should be delivered immediately.
The treatment of the baby for GBS would follow the charity’s normal paediatric recommendations.
Our Medical Advisory Panel’s recommendations for stopping GBS infections in newborn babies are the same for home births and births in freestanding midwifery units as for hospital births – women whose babies are at higher risk of developing early-onset GBS infection should be offered intravenous antibiotics from the start of labour until delivery.
If you want to give birth at home or in a freestanding midwifery unit and have the intravenous antibiotics during labour until your baby is born, do discuss this with your medical team. It may be possible for your midwife to give you IV prescribed for you by your GP. However, this is not widely available. Some areas won’t permit IV to be given at home or in a freestanding midwifery unit – there is a small risk that you would get a severe allergic reaction to the antibiotics and, obviously, there is no intensive care unit nearby. The risk is small and the antibiotics make the chance of the baby developing group B Strep infection much smaller, but your health professionals may be anxious. Of course, around 20-25% of women giving birth n these locations are likely to be carrying GBS when they give birth without knowing it.
Oral antibiotics are not recommended for women for GBS carriage during pregnancy or labour. There’s no evidence that they prevent GBS infections in babies. [If you want a home birth and it’s not possible for you to have the IV antibiotics at home, you may wish to consider having intramuscular antibiotics. However, our Medical Advisory Panel does not recommend these instead of the IV antibiotics during labour, but they may be better than nothing if that really is the only alternative.
There is evidence that group B Strep does cause late miscarriage and stillbirth, as well as being implicated in preterm birth. However, we don’t know of any evidence that GBS causes earlier miscarriages.
Group B Strep can cause infection in a baby in the womb, which can result in problems before the baby is born, these events are not common and GBS is a rare cause of them. For a baby to develop a group B Strep infection before birth, ALL of the Mum’s and the baby’s various defence mechanisms need to have failed. And there really are quite a lot of natural defences – in the vaginal secretions, the mucous plug, the cervix, the amniotic membranes, the amniotic fluid and finally in the baby him/herself. With so many defences in place, against group B Strep, thankfully the large majority of babies are not affected by group B Strep. For more information, visit our Group B Strep and Stillbirth page.
If a woman has had any gynaecological or obstetric problems, or other infections, etc in the past, it’s important that these are investigated fully by a Consultant Obstetrician at booking (or before) as well as addressing the issue of GBS.
If GBS has been detected during the current pregnancy from swabs or the urine, or if Mum has previously had a baby who developed GBS infection, then Mums should be offered intravenous antibiotics as soon as possible once labour has started.
If there are any concerns about anything during pregnancy (including, for example, reduced fetal movements which can be a sign that the baby is in distress), the Mum should seek advice from her midwife in the first instance. If she’s not available, then she should contact her maternity unit – they’re there to help.
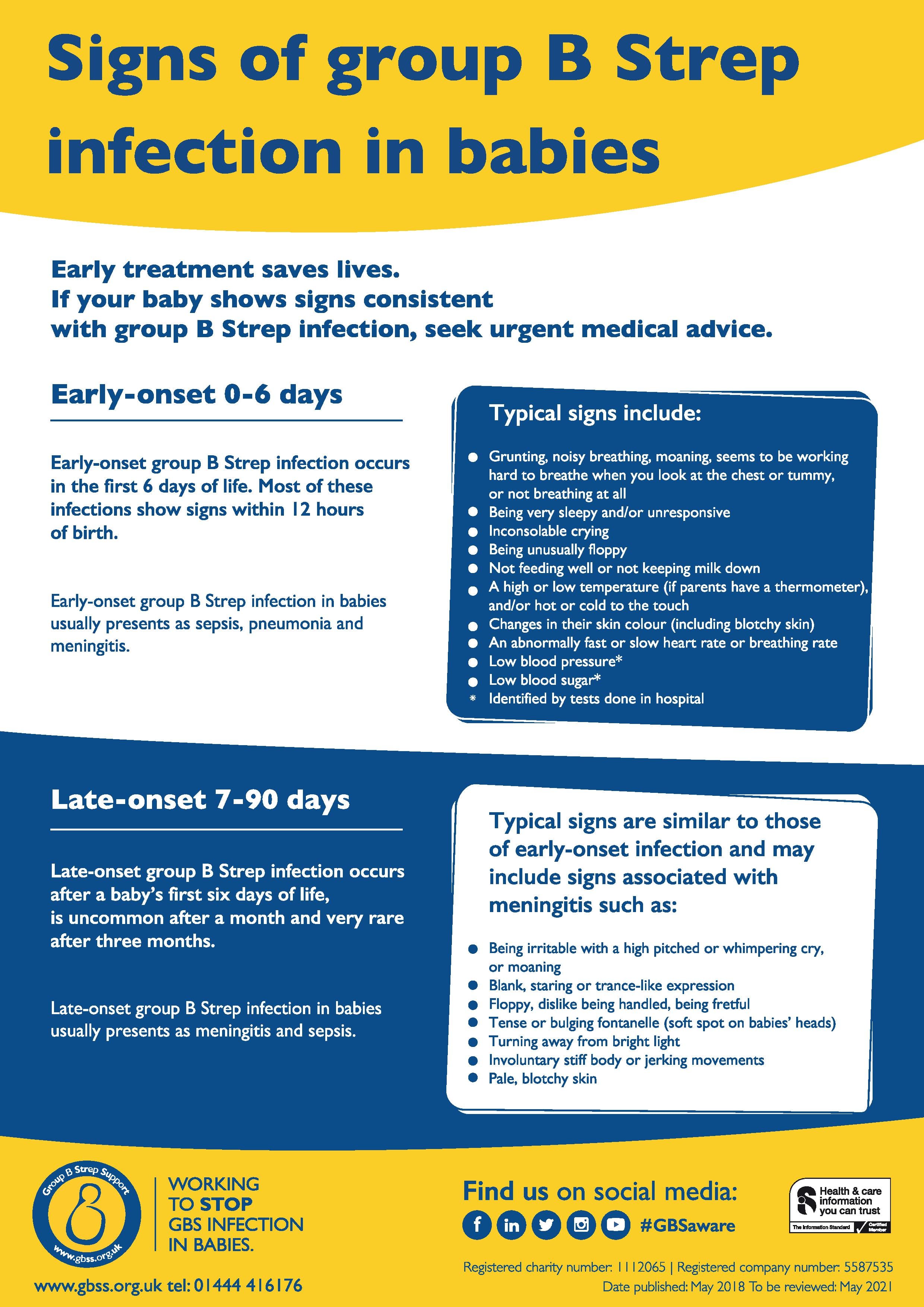
Most babies who develop group B Strep infection become unwell in the first week of life, usually within 12 to 24 hours of birth. This is known as early-onset group B Strep (EOGBS) infection. Most of these EOGBS infections may be prevented with intravenous antibiotics given in labour to mothers who are carrying group B Strep or who have other recognised risk factors.
Babies can also develop group B Strep infection from 7 days old up to three months old. This is known as late-onset group B Strep (LOGBS) infection and is less common than EOGBS infection. Having intravenous antibiotics during labour does not prevent LOGBS infection.
You can download our poster highlighting the most common signs of group B Strep infection in babies here and read more about the signs of GBS infections on this page.
Our medical advisory panel strongly recommends you should be encouraged to breastfeed your baby. Although there have been isolated cases describing group B Strep infection, possibly related to breast milk contamination, the advantages of breastfeeding will, in our medical advisory panel’s opinion, greatly outweigh the remote risk of transmitting GBS via breastfeeding.
High hygiene standards need to be maintained for all breastfeeding mothers, with the hands and nipple areas being kept clean.
The intravenous antibiotics recommended for pregnant women during labour and at intervals until the baby is born to protect the newborn baby from GBS infection are safe for breastfeeding mothers, although you should make sure your medical professionals know you intend to breastfeed your baby.
If you develop mastitis or a breast abscess, you should seek medical advice regarding breastfeeding.


{kind=link}